|
PATHOPHYSIOLOGY
The colon is made up of four layers: the mucosa, the submucosa, the muscularis, and the serosa. The mucosa and submucosa are divided by the muscularis. Reproduction of cells in the colon takes place in the crypts of Lieberkuhn located in the mucosal layer. As new cells are produced, old cells mature, migrate out of the crypt, and shed. Damage to the crypts will affect reproducing cells and the crypts become prone to errors and to the formation of early adenomas.21
The large intestine consists of the cecum, ascending colon, transverse colon, descending colon, sigmoid colon, and rectum. The ascending colon, descending colon, and rectum are considered extraperitoneal organs because the ascending and descending colon lie in the anterior pararenal space and are covered by a single layer of the posterior peritoneum. The rectum is surrounded by extraperitoneal perirectal fat in the pelvis. The transverse and sigmoid colon are suspended in the peritoneal cavity by the mesocolon that is formed by two layers of peritoneal linings. The cecum is attached to the ileocolic mesentery in the right iliac fossa. The arterial supply to the cecum, ascending colon, and transverse colon derives from the superior mesenteric artery, whereas the blood supply to the sigmoid colon, descending colon, and upper rectum is from the inferior mesenteric artery. The lower rectum is supplied by the internal iliac arteries. The superior mesenteric vein drains the cecum, ascending colon, and transverse colon. The artery and vein supplying and draining each segment of the colon accompany each other in the mesocolon. The venous system of the colon and upper rectum drains into the portal circulation.21 The distal 5-7 cm of the rectum has a dual drainage.
Nodal spread from each segment of the colon follows the blood vessels in the mesocolon.22 Invasion of the venous system yields a poor prognosis. Once tumor cells invade the vascular system, widespread dissemination of the disease follows; it is not amenable to surgical resection and the effect of chemotherapy and radiation therapy is limited. Local invasion into the neighboring structures is more common in the cecum and rectosigmoid areas. The liver is the most frequent site of metastatic involvement. Solitary pulmonary metastasis is rare. Other areas of metastasis include the brain (cerebellum), bones, kidneys, and adrenals.21 By the time of the diagnosis, approximately 25% of the colon cancers will have extended through the bowel wall; whereas cancers of the rectum will have spread through the wall in 50%-77% of patients and will have metastasized to lymph nodes in 50%-60% of cases.2 Distal rectal cancers are likely to produce isolated pulmonary metastasis.1 Implantation of tumor cells at other sites can occur as a result of surgical manipulation of the tumor, intraluminal spread, or the shedding of tumor cells into the peritoneum. Intraperitoneal seeding and carcinomatosis may occur even without lymphatic or visceral spread.
The most common histological type of colorectal cancer is adenocarcinoma. Others, which are rare, include lymphoma, sarcoma, melanoma, and carcinoid. Adenocarcinoma accounts for over 90% of all large bowel cancers. Mucin adenocarcinoma is a variant characterized by increased amounts of extracellular mucus in the tumor. Signet ring cell carcinoma is characterized by large amounts of intracellular mucin material that cause the cytoplasm to displace the nucleus.2 Squamous cell carcinomas, carcinoid tumors, and adenosquamous and undifferentiated carcinomas have been found in the colon and rectum as well.2 Whereas previously the most common sites of colon cancers were the sigmoid and descending colon, now the proximal colon is the site of highest incidence.
The anus is the terminal 4-6 cm of the gastrointestinal tract. It is responsible for maintaining continence. The anal canal is that region extending from the anal verge to the junction between squamous and columnar epithelium. Another way of describing this area is the area between the anal verge and the anorectal ring. The anorectal ring is easily palpable and corresponds to the junction of a portion of the levator muscle with external anal sphincter. The spread of anal and perianal cancers can be predicted based on the anatomy since the tumor usually spreads by direct extension, through the lymphatic system, and via the bloodstream. Tumors may spread upward for 5-6 cm before ulcerating into the rectum.21 Most anal cancers are squamous cell carcinomas. Other less-common cell types are cloacogenic, basaloid, transitional, and mucoepidermoid carcinomas.2 Unusual tumors arising in the anal canal include small-cell carcinomas, melanomas, and lymphomas. Small-cell carcinomas of the anal canal are aggressive and signal early distant metastases.3
Adenocarcinomas of the colon and rectum develop initially in the mucosa. The tumor then locally invades into the lumen of the bowel wall. When it has traversed the muscularis mucosa and infiltrated the submucosa, it is termed invasive. Further infiltration by way of the lymph and vascular system occurs next and direct extension may occur into the peritoneal surfaces as well.
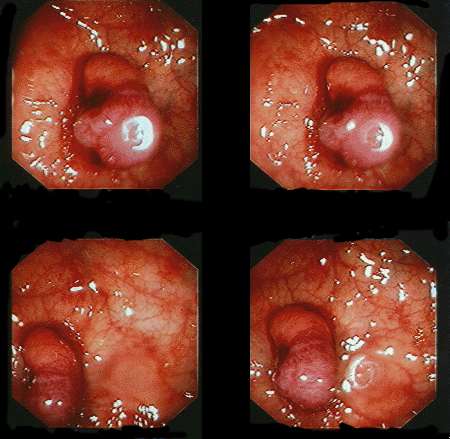
Depending on their location in the bowel, colorectal lesions may exhibit different characteristics. Tumors in the ascending colon present as cauliflower-like fungating masses that progress to become ulcerative and necrotic. These are usually well differentiated and have a better prognosis. Tumors in the descending and sigmoid colon present as ulcerative tumors that tend to infiltrate the bowel wall and have a poorer prognosis than those in the ascending colon. Rectosigmoid tumors present as villous, frond-like lesions.
Review of Key Points:
- The most common histological type of colorectal neoplasm is adenocarcinoma.
- The most common anatomical sites affected are the descending and sigmoid colon.
- Colorectal lesions exhibit different characteristics depending upon their location in the bowel.
- Right-sided tumors present as cauliflower-like fungating masses that progress to become ulcerative and necrotic are usually well differentiated and have a better prognosis.
- Left-sided or descending sigmoid colon lesions present as ulcerative tumors with everted edges. These tumors tend to infiltrate the bowel wall and have a poorer prognosis than right-sided tumors.
- Rectosigmoid tumors present as villous, frondlike lesions.
- Early rectal cancer symptoms include a change in the caliber of the stool and rectal bleeding. Advanced cancer symptoms include tenesmus and rectal pain.
- Adenocarcinoma of the colon and rectum develops in the bowel mucosa. The tumor will invade locally usually by direct extension protruding into the lumen of the bowel wall.
- Once the tumor has traversed the muscularis mucosa and infiltrates the submucosa, it is termed invasive.
- The major site for visceral spread is the liver.
- The median survival for individuals with distant metastasis ranges from six to nine months.
CLINICAL MANIFESTATIONS
Clinical manifestations of tumors in the colorectum vary depending on location. Tumors in the ascending colon are usually large and bulky. Symptoms generally include anemia, a palpable mass in the right lower quadrant, and a vague, dull pain. Cancer of the transverse colon is generally noted by a change in bowel habits and blood in the stool. Symptoms of cancer of the descending and sigmoid colon again depend on the type of growth typical of this area. Cancer of the rectum is usually manifested as bright-red bleeding, symptoms of incomplete evacuation, and tenesmus. The sensation of a mass in the rectum is often mistakingly attributed to hemorrhoids or anal fissures and may require a rectal examination and biopsy for accurate diagnosis. A proctosigmoidoscopy will provide an adequate examination to secure biopsy and provide a baseline for surgical assessment. Instructing the patient, assisting with the examination, and providing support and privacy for the patient during the procedure are crucial to a successful examination.
Clinical signs and symptoms that may be present in patients with colorectal cancer include the following:2,23,24
- Early cancer: Asymptomatic; vague abdominal pain and flatulence, minor changes in bowel movements with or without rectal bleeding.
- Late cancer: Severe pain, anorexia and weight loss, sacral or sciatic pain, and jaundice, pruritis, ascites, hepatomegaly, renal impairment.
- Descending/sigmoid: Constipation alternating with diarrhea, abdominal pain, and obstructive symptoms (nausea/vomiting), melena, perforation.
- Ascending: Vague abdominal aching discomfort, anemia, weakness, weight loss, right-sided abdominal mass, fatigue, palpitations, change in stool.
- Rectal: Changes in bowel movement, rectal fullness, urgency, bleeding, tenesmus, jaundice, malaise, occult blood, pelvic pain.
- Anal: Bleeding, discharge, rectal mass, tenderness on palpation, pain on defecation.
- Transverse: Constipation alternating with diarrhea, bowel obstruction, melena.
|
